Knee Anatomy 101
Bone Basics
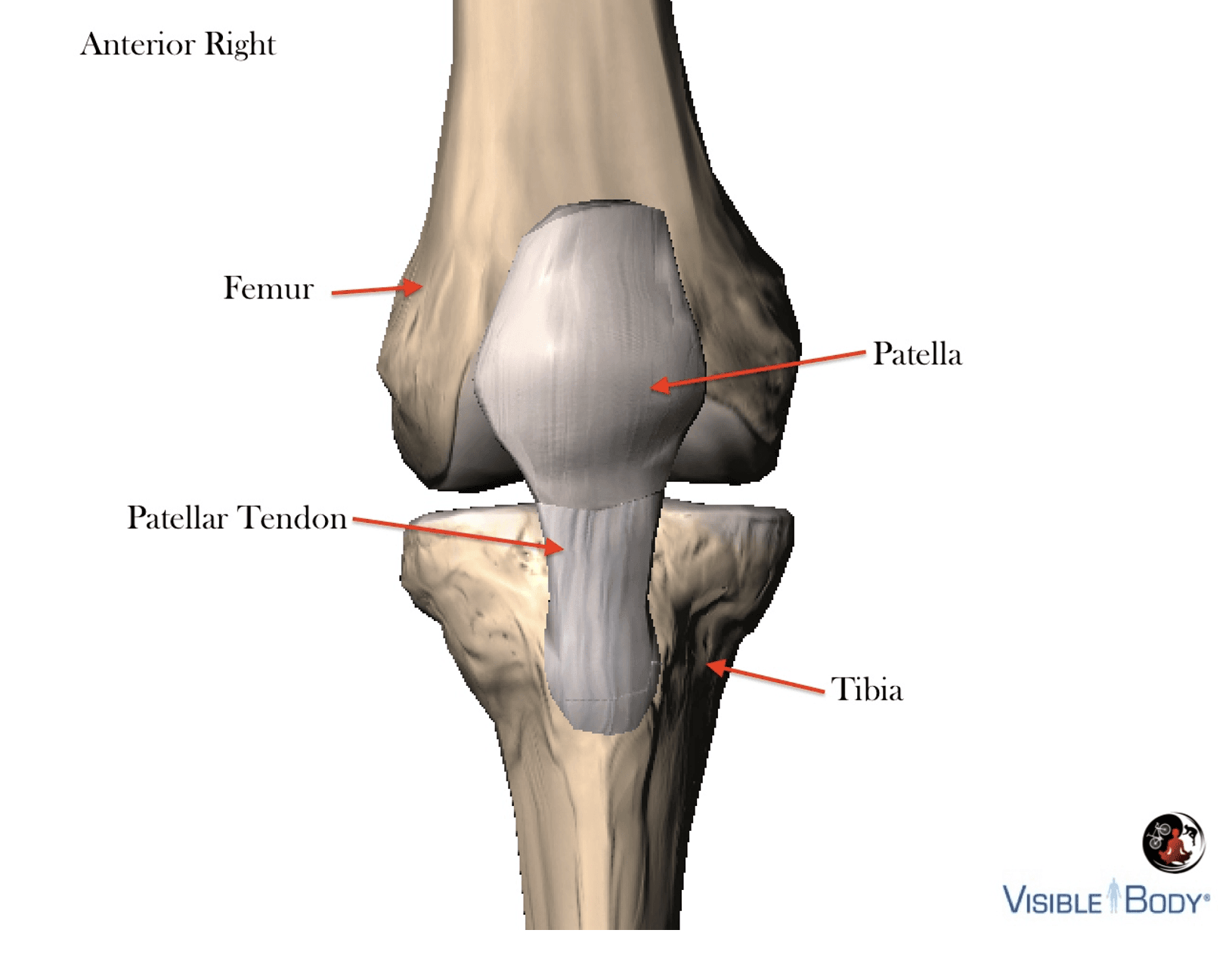
There are three bones at the knee joint – femur, tibia and patella – commonly referred to as the thighbone, shinbone and kneecap. The fibula is not typically associated with the knee because it lies outside the capsule and as associated with ankle function.
We need to consider the osteological features (study of bones) of this joint to fully appreciate the numerous complex movements necessary to accomplish flexion and extension.
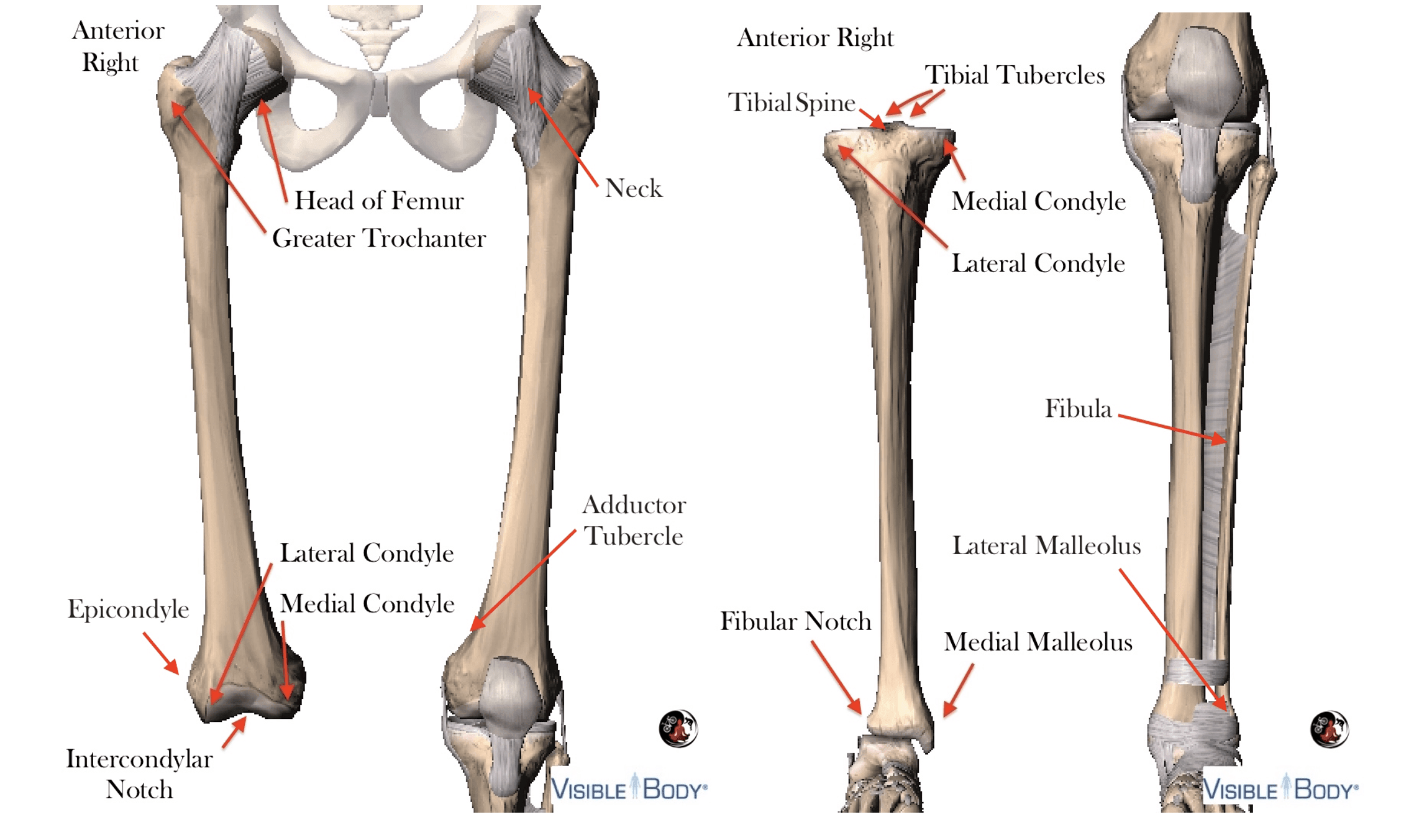
The femoral head sits inside the acetabulum at the ball and socket hip joint with the neck connecting laterally to the greater trochanter.
Distal features include the convex medial/lateral condyles, Intercondylar notch or patellar groove and adductor tubercle.
The femur articulates at the tibial plateau. These condyles are concave medially, convex laterally, and divided by the tibial tubercles, which fit snugly into the Intercondylar notch in extension.
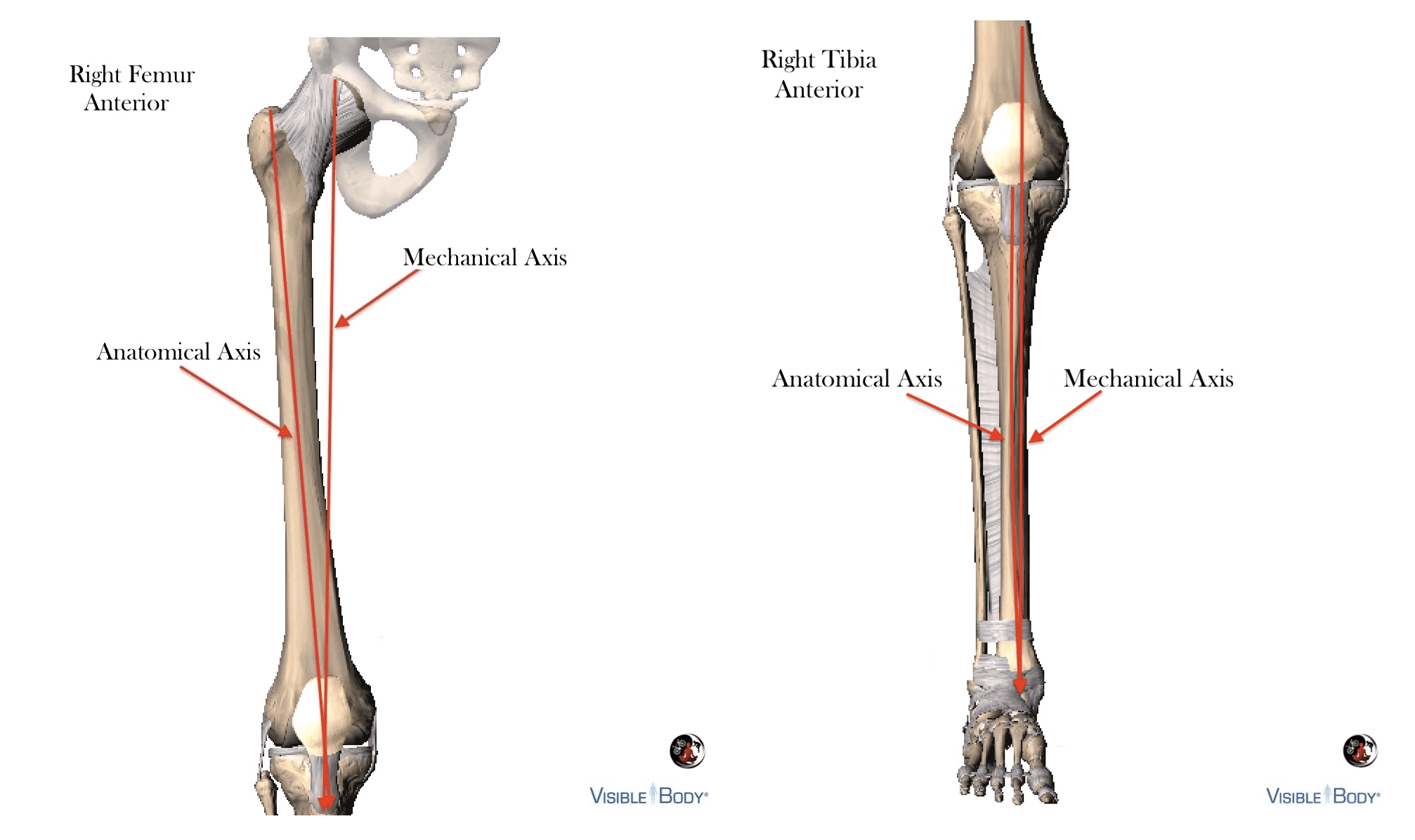
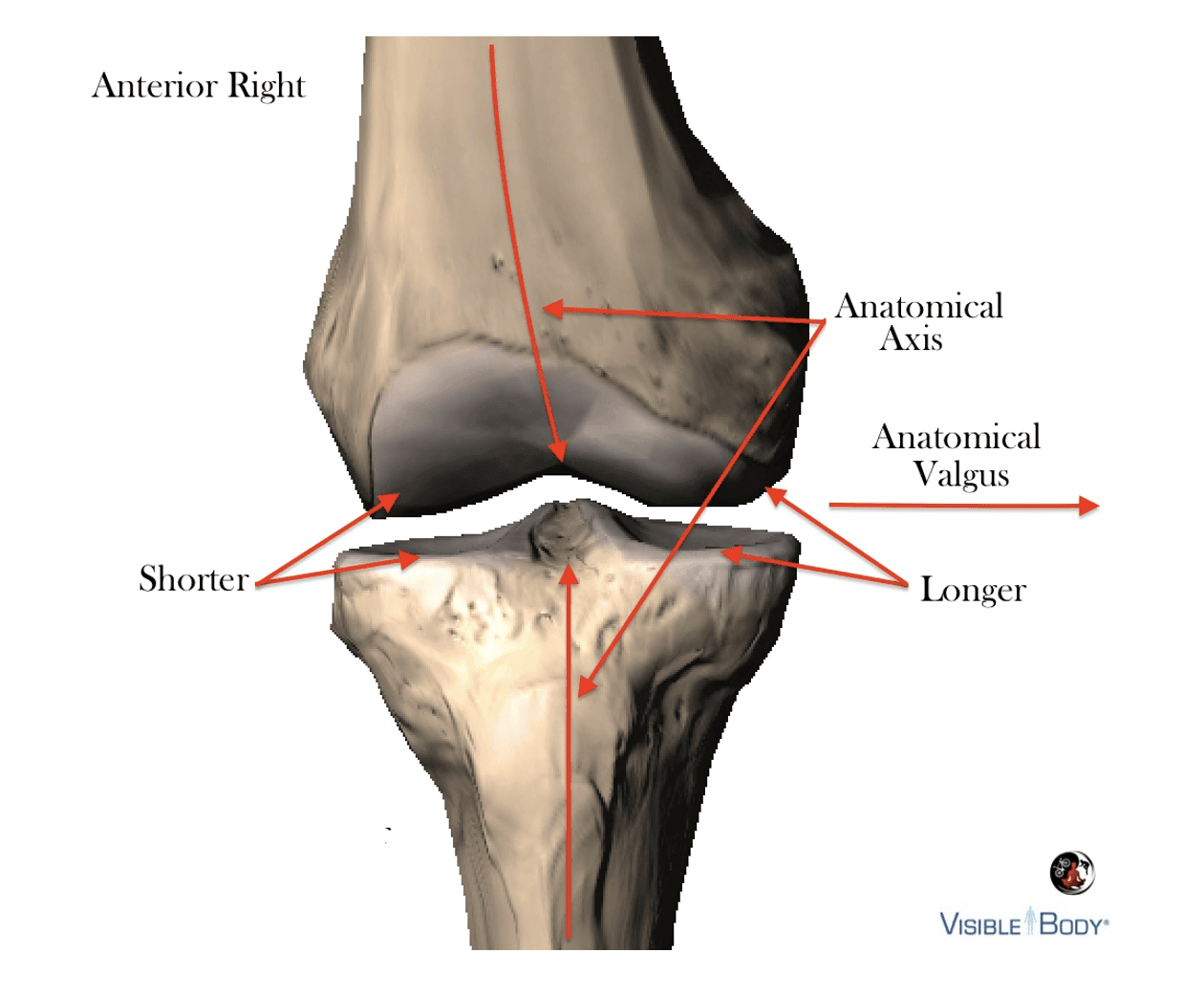
The anatomical axis of the femur bone is divergent from the mechanical axis, descending medially from the center of the greater trochanter to the Intercondylar notch; conversely, the anatomical and mechanical tibial axis are nearly identical. Many fitters try to align the mechanical axis with the cycling cleat when fitting, which seems logical, but in practice the anatomical axis is equally important.
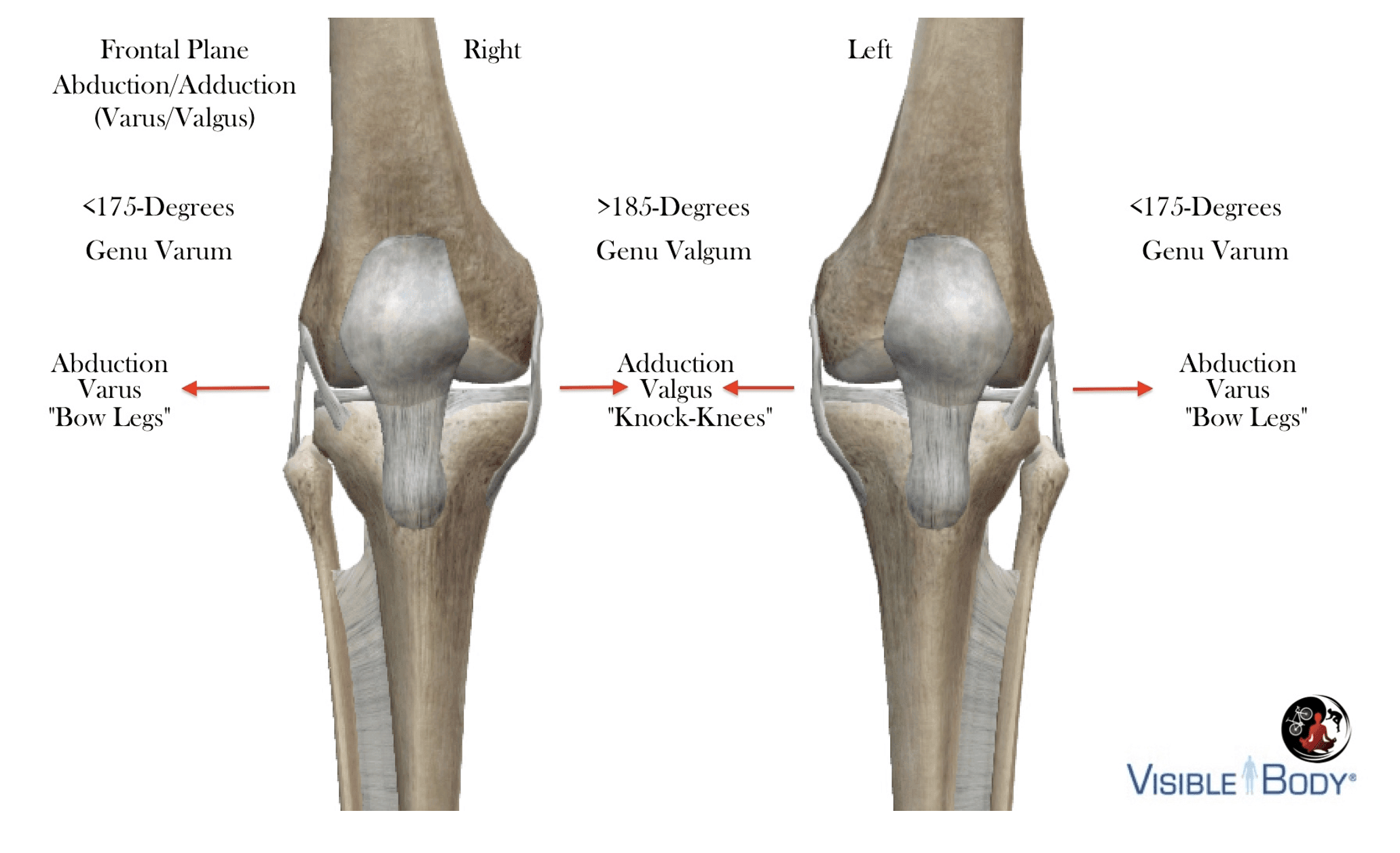
Close examination of the tibial and femoral medial condyles of both femur and tibia extend further than their respective counterparts, which creates a physiologic valgus angle of the knee approximating 180- 185-degrees. It is normal for the knee to travel in a valgus orientation during extension because it is driven by joints — not muscles.
Diagnostic criteria for abnormal frontal plane adduction is >185-degrees (Genu Valgum) or </= 175- degrees abduction (Genu Varum), measured at the medial-tibiofemoral joint in extension. Trying to correct anatomical valgus with shims can increase medial compartment compression which can have has a negative impact on vastis medialis recruitment.
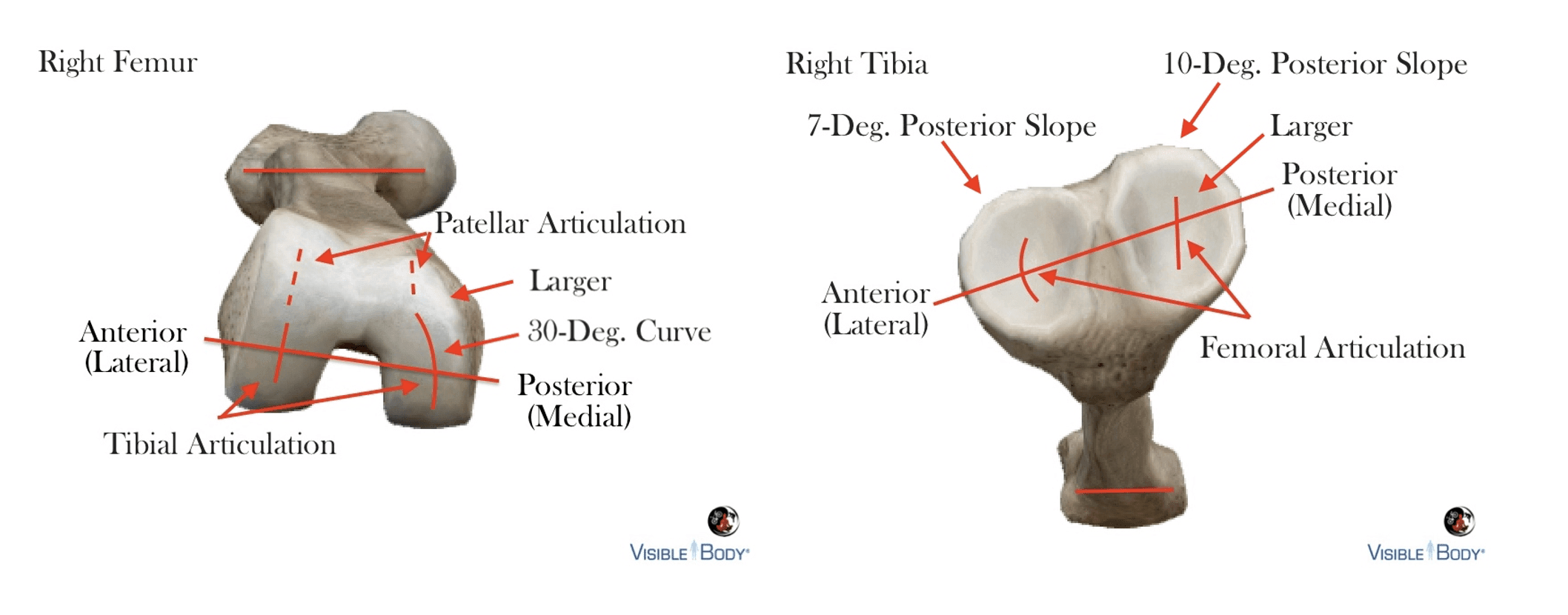
The anterior orientation of both lateral condyles and a 25-30-degree curve on the medial femoral condyle are probably the most distinct features of the tibiofemoral articulating surface structure.
The medial femoral condyle articulating surface area is larger and curved relative to the lateral condyle, which is flatter, smaller and more circular. Both structures are convex.
At the tibial plateau, the medial condyle is concave and 50% larger than the partially convex lateral condyle. The degree of posterior slope varies between condyles, as does the amount of cartilage. We can see from the diagram that most of the rotation/spin occurs at the lateral condyle.
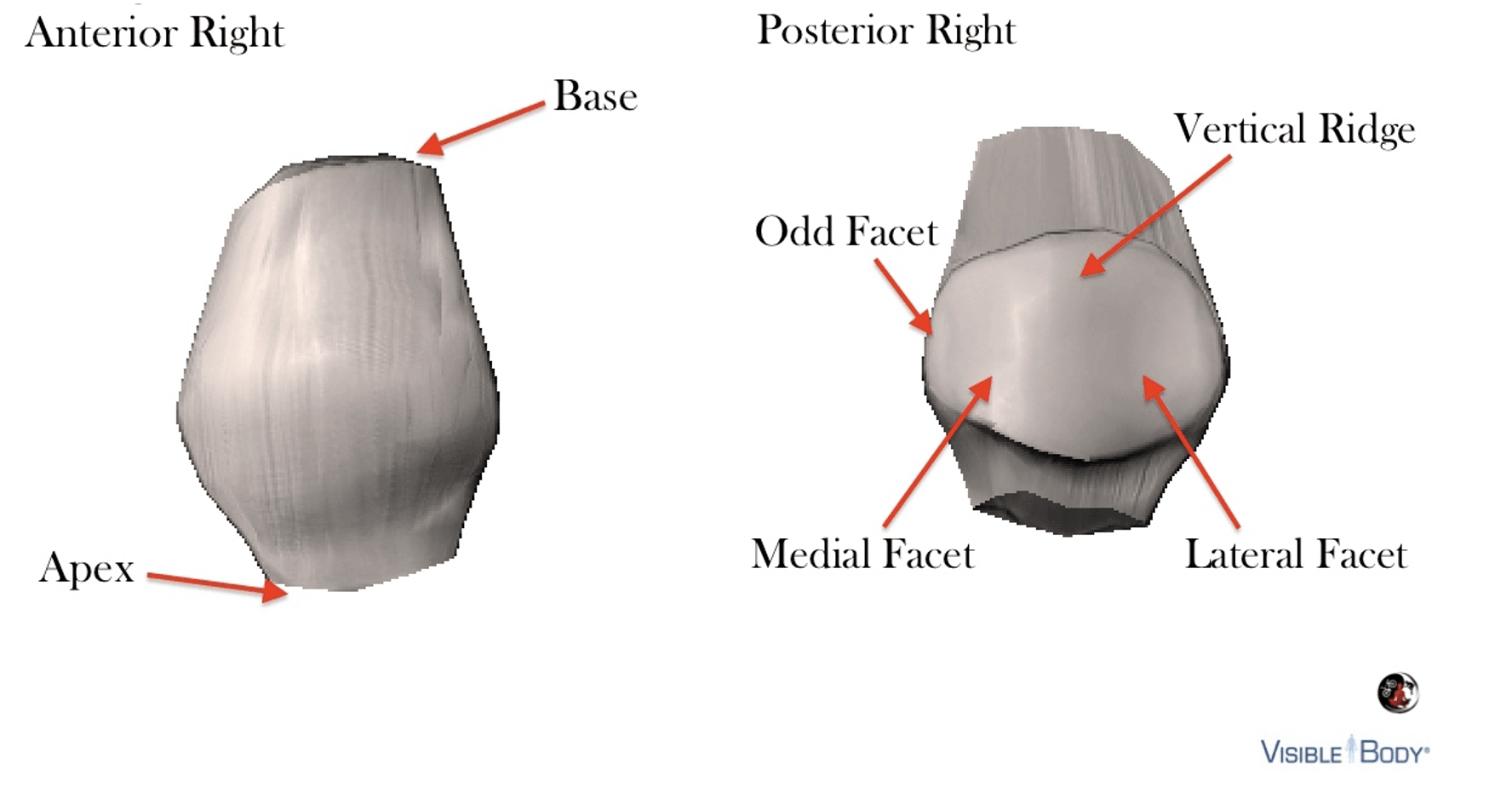
 The patella is embedded within the retinacula layer between the femur and tibia, attached superiorly to the quadriceps tendon and inferiorly to the patellar tendon. Exposed posteriorly to articulate with the femoral sulcus, the surface contains a central vertical ridge and facets. There is significant compression between this bone and the femur during extension.
The patella is embedded within the retinacula layer between the femur and tibia, attached superiorly to the quadriceps tendon and inferiorly to the patellar tendon. Exposed posteriorly to articulate with the femoral sulcus, the surface contains a central vertical ridge and facets. There is significant compression between this bone and the femur during extension.
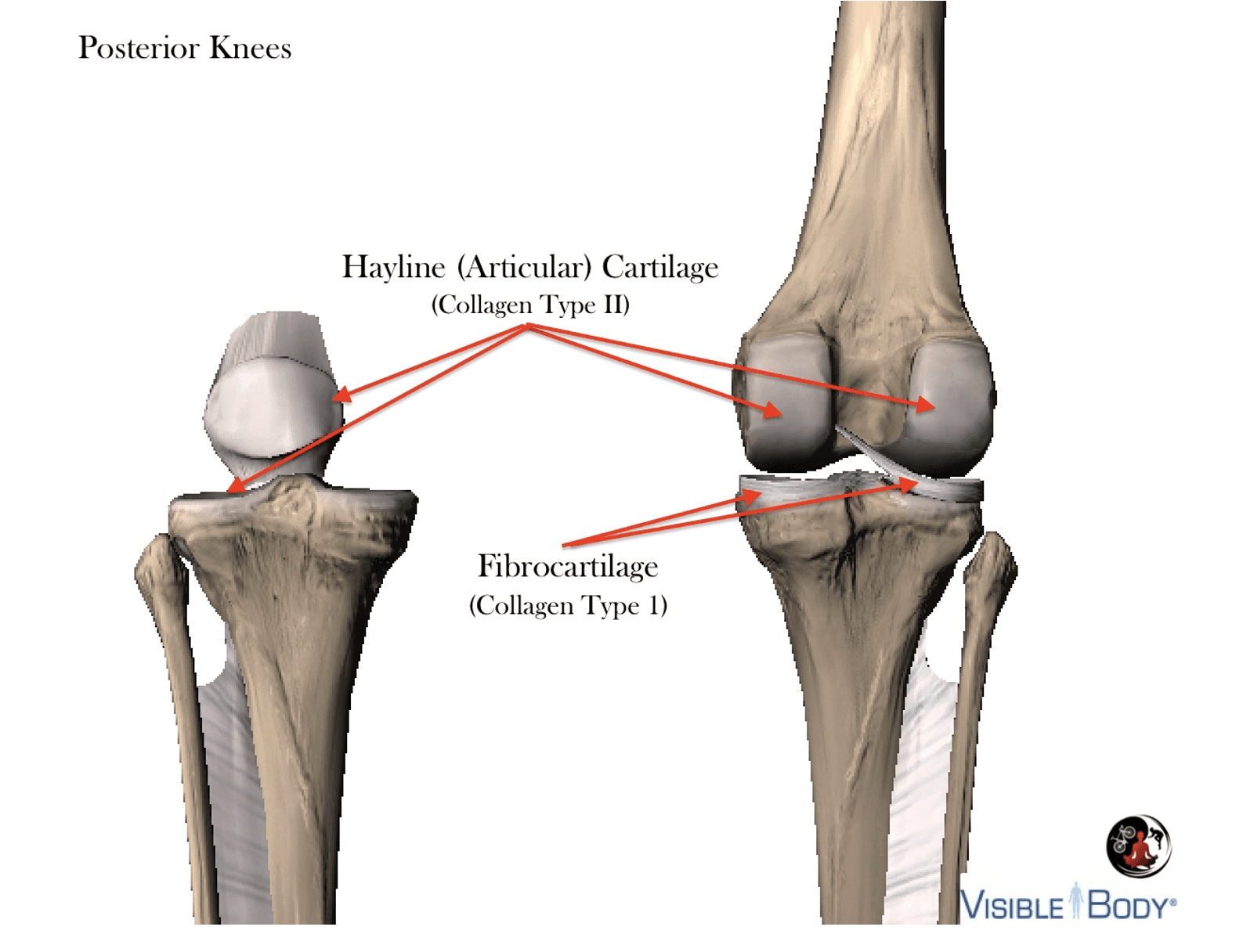
Cartilage Basics
Hyaline cartilage covers a large portion of the femoral condyles and posterior patella to reduce patellofemoral articular friction.
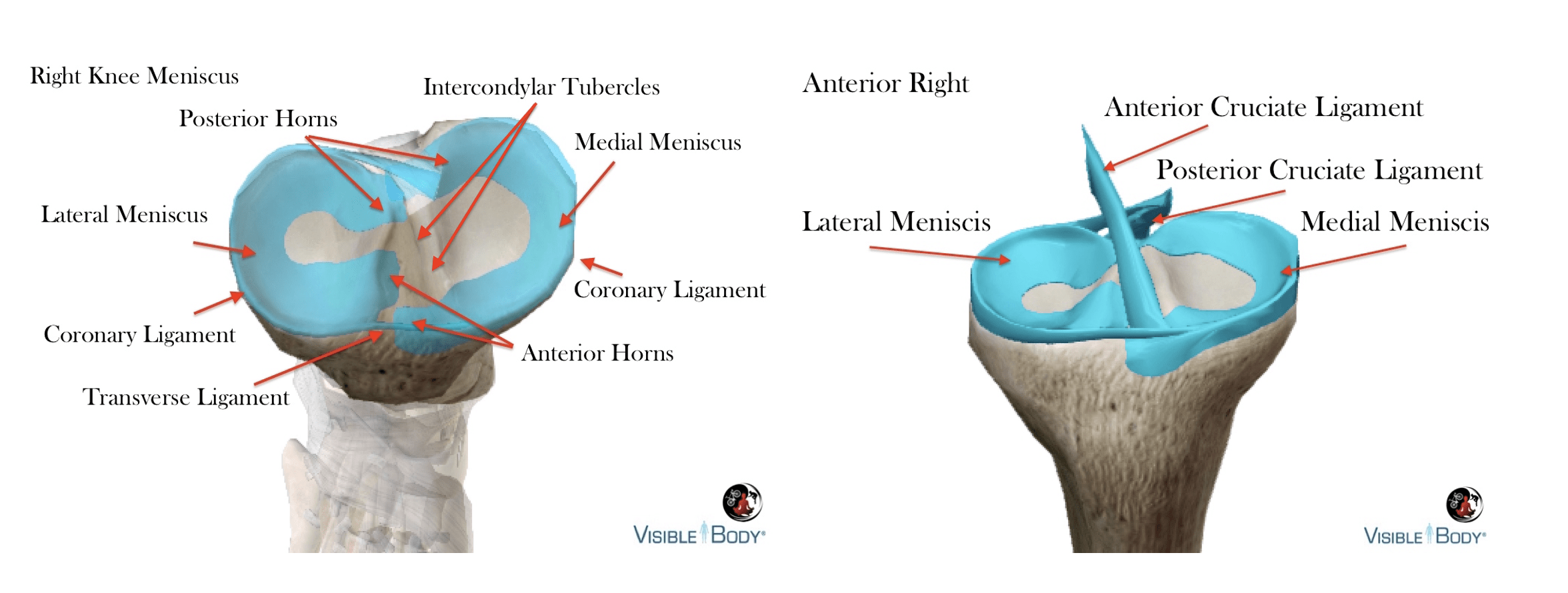
Fibrocartilagenous menisci at the tibial plateau create a semi-flexible housing that compensate tibiofemoral obliquity.
Menisci attached to the surface of the tibial plateau improve congruence, pressure distribution and articulation at the tibiofemoral joint. There are studies suggesting a more posterior saddle increases tibiofemoral compression, but this is nearly insignificant compared to the forces when standing, walking, etc.
Fixed to the tibia at the horns and coronary ligaments they are joined anteriorly by the transverse ligament.
The lateral meniscus forms a nearly complete circle and covers a majority of the tibial condyle’s surface, with anterior and posterior horns (typically) blending into the attachment of the ACL. There is no attachment between the lateral meniscus and the lateral collateral ligament, providing increased mobility in comparison to the medial meniscus.
The c-shaped medial meniscus is larger, but covers significantly less surface area then the lateral meniscus. Anterior fibers of the ACL blend with the transverse ligament and anterior horn of the medial meniscus. And capsular attachments join to the deep medial collateral ligament directly and patella via the patellomeniscal ligaments.
Ligament Basics
Ligaments create passive resistance to facilitate optimal knee function and stability.
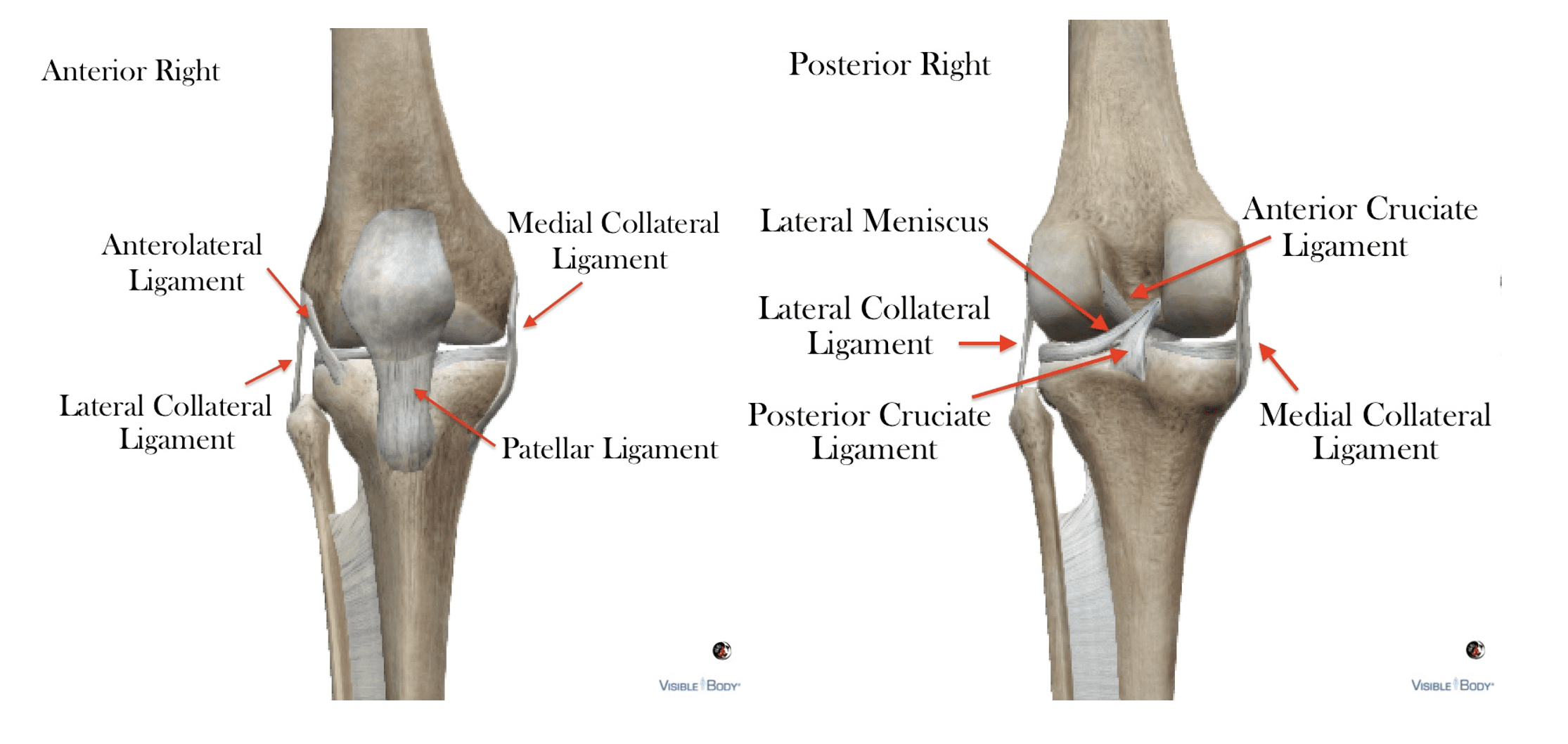
Tibiofemoral Ligaments:
The deep anterior and posterior cruciate are considered Intracapsular and extra synovial because they exist inside the joint capsule but outside the synovial membrane, crossing anterior/posterior & posterior/anterior between femur and tibia.
The medial (tibial) collateral ligament contains superficial (extracapsular) and deep (capsular) components, between femur and tibia, and the lateral (fibular) ligament is purely extracapsular, connecting femur to fibula.
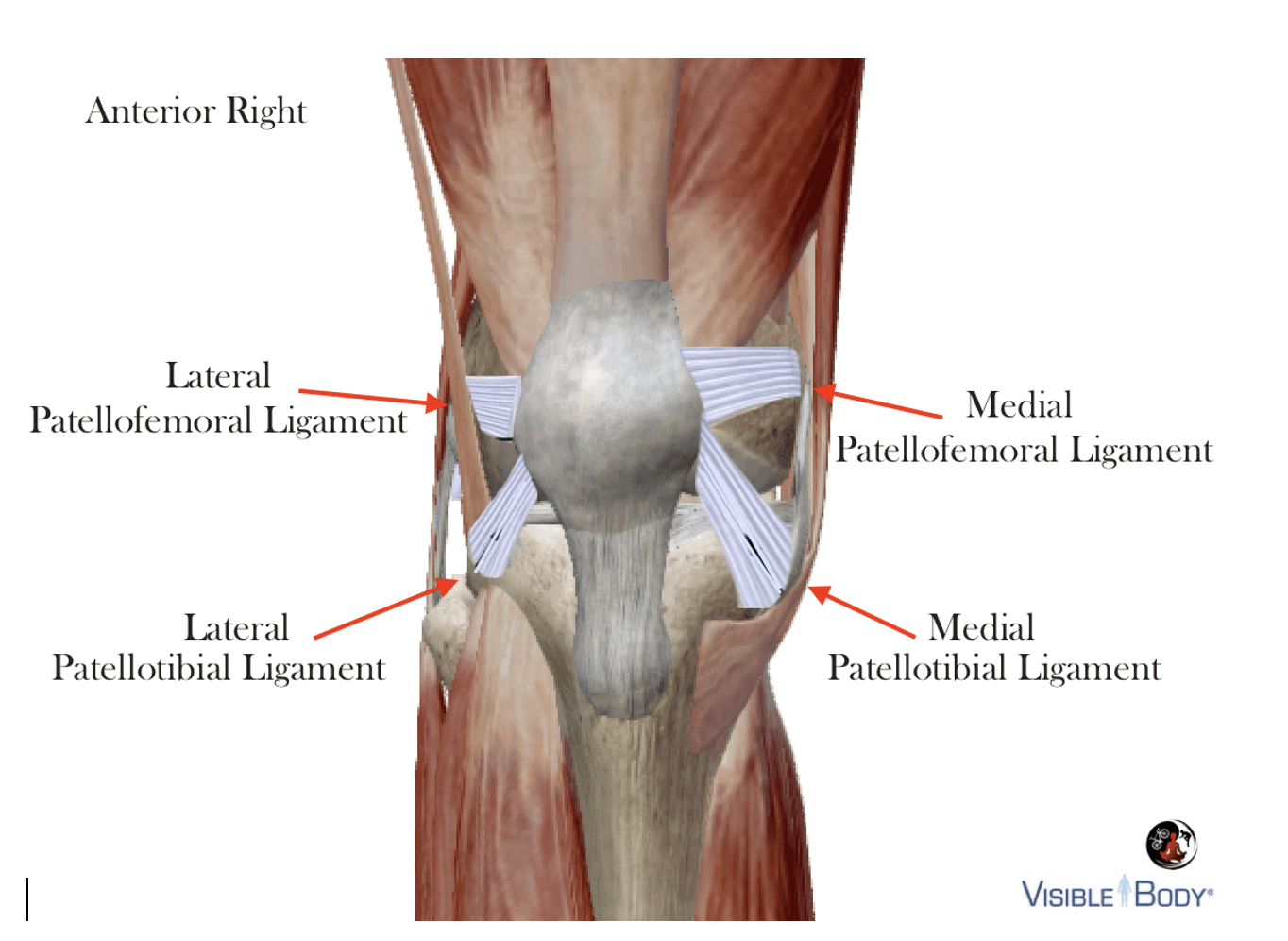
Patellofemoral Ligaments
Patellar movement is initiated by the quadriceps and guided by the medial/lateral tibial and femoral ligaments. These ligaments are implicated in patellar tracking issues, but not to the same extent as muscle imbalances.
Knee Joint Capsule
Consistent with other synovial joints, the knee exists within a capsule made of connective tissue and bone.
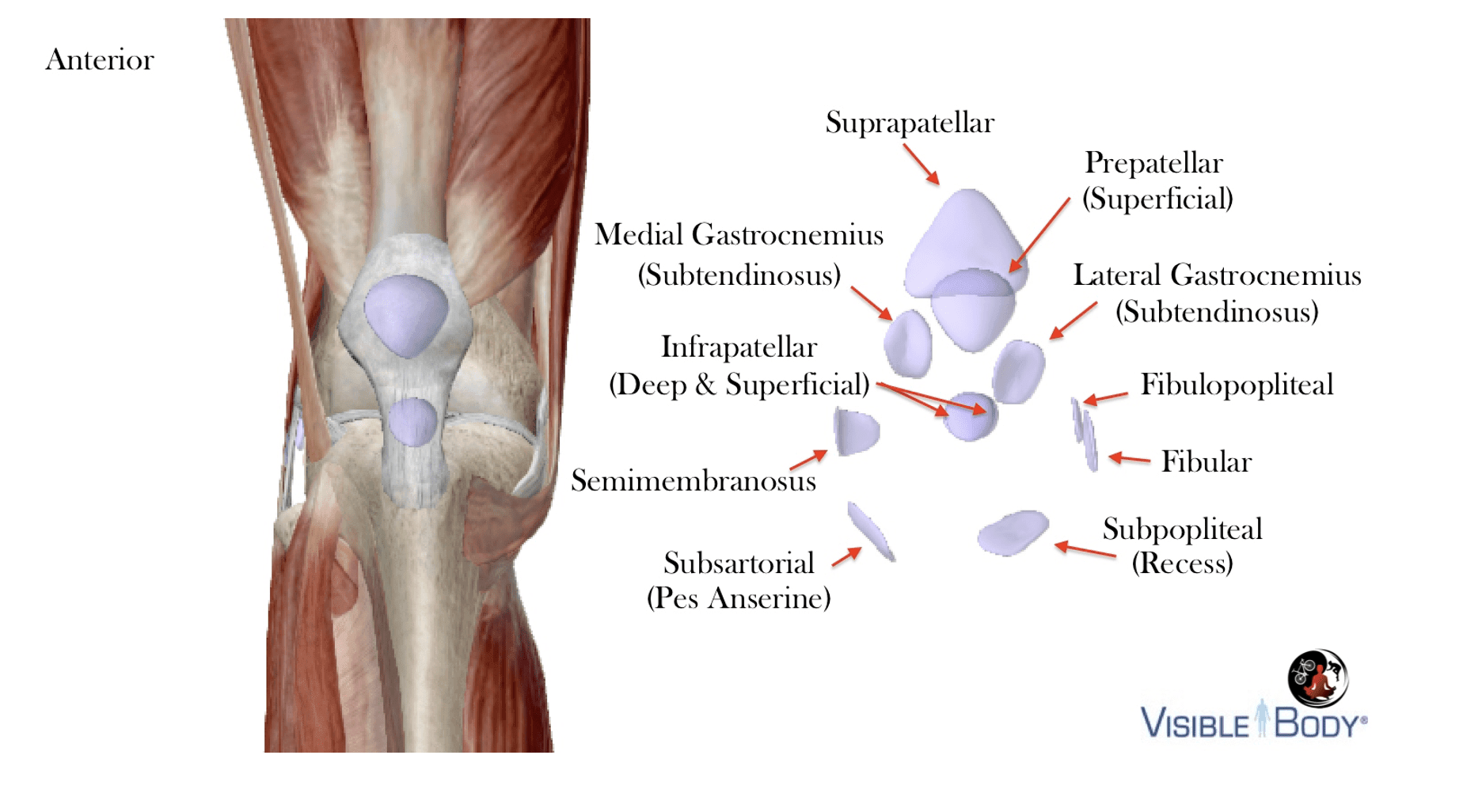
The outer layer consists of a fibrous membrane with openings at the patella for the suprapatellar bursa and lateral tibial condyle for popliteal muscle, inseparable with numerous supporting capsular ligaments.
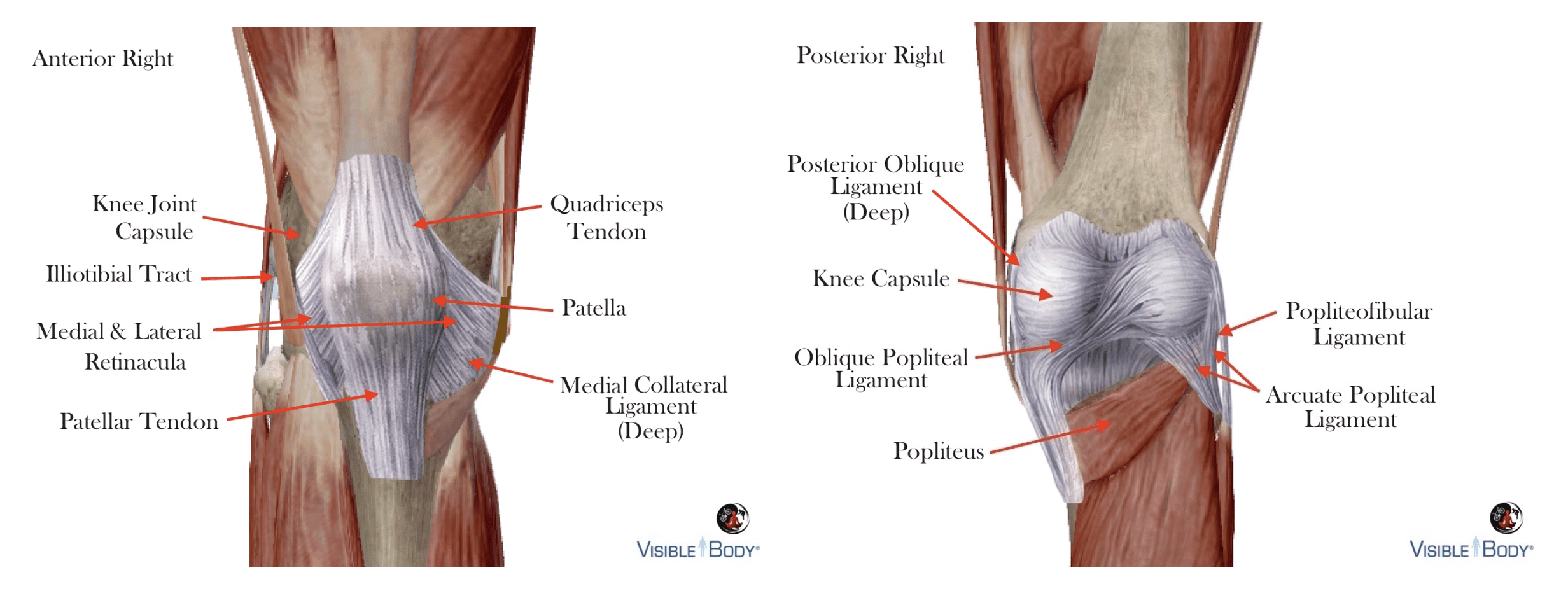
The inner-membrane secretes synovial fluid (and nutrients) to reduce friction between joint surfaces
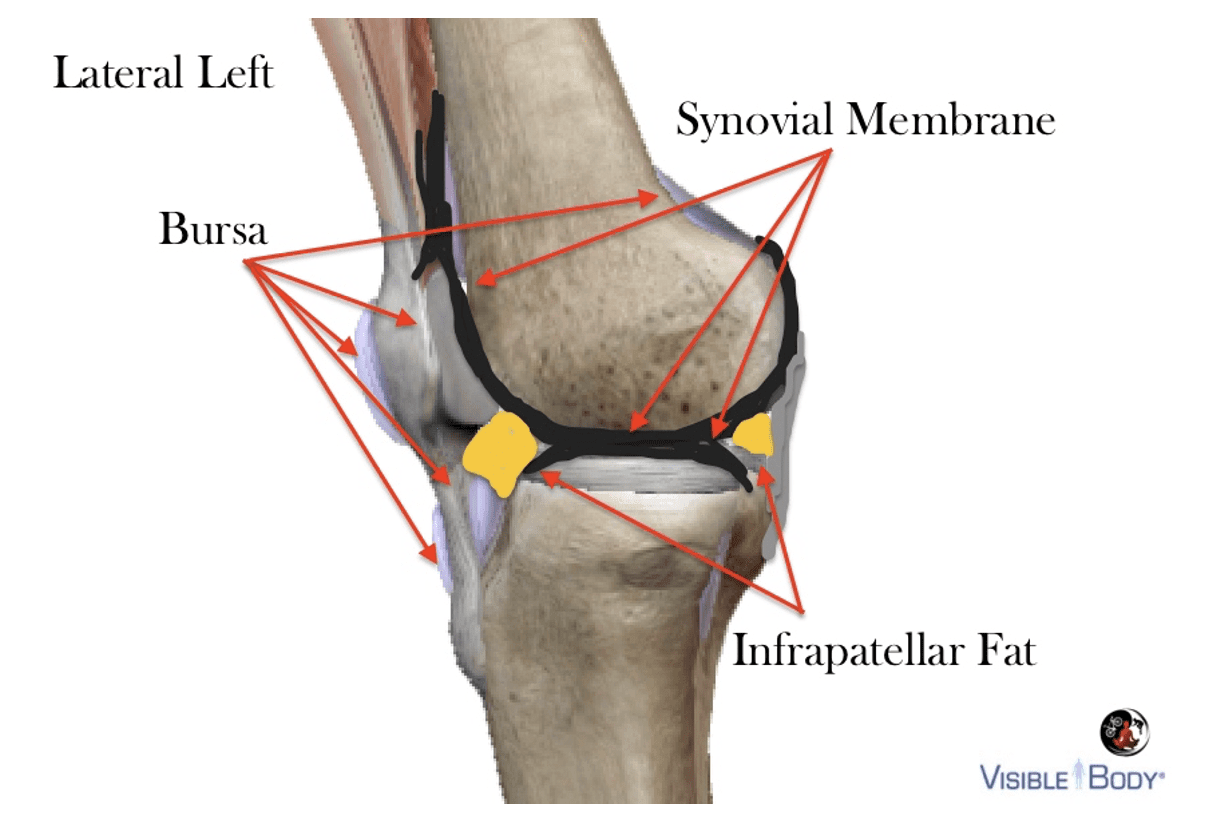
Bursa and fat-pads are interspersed between muscles, tendons and bones as buffers for friction and pressure.
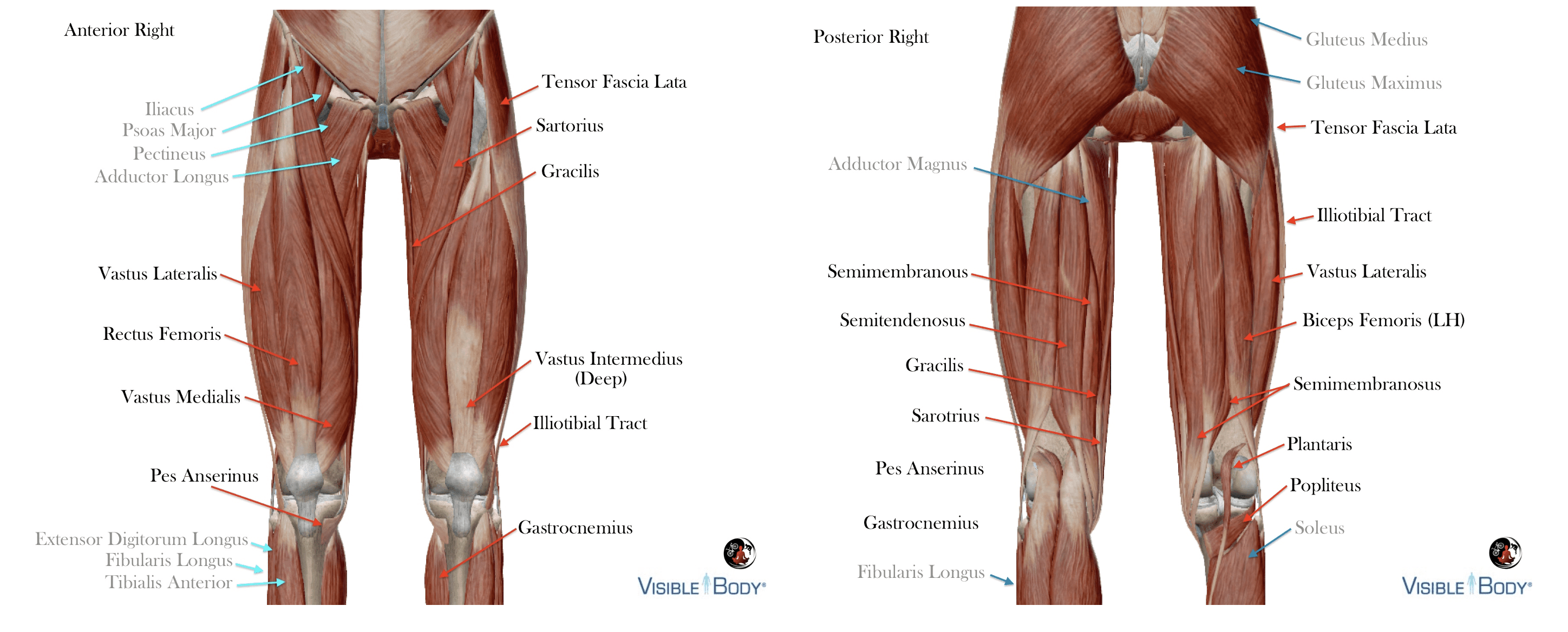
Muscle Basics
Anterior muscles of knee joint are monoarticulating (articulate/cross one-joint) or biarticulating (articulate/cross two-joints). Muscles indirectly influencing the knee are indicated with blue arrows. Posterior muscles of the knee joint are also mon0- and biarticulating. Muscles indrectly impacting the knee are indicated with blue arrows.